At Compassion in Dying we want people to be in control of their end-of-life decisions, because there is no-one better to make them.
Everything we do starts with what dying people tell us. We listen to what they say and amplify their voices. We shift attitudes and drive changes to the healthcare system, so people’s end-of life decisions are heard, understood and respected when it matters most. And we support people to make informed choices, start honest conversations about death and dying, and record and revisit their wishes whenever they want to.
Acknowledgements
Thank you to all the people who have shared their experiences so passionately and generously. Your voices are an important force for change.
People’s voices matter. The challenge is this: how can we ensure that those voices are sought, heard, and reflected in our decisions and actions?
Vinnie Nambisan, Consultant in Palliative Medicine and Trustee of Compassion in Dying
Foreword
I have seen a remarkable shift in healthcare culture since my palliative care career began more than 20 years ago. With increasing recognition that our role is more than just treating a patient’s illness – it is also to care for the person in front of us. With that comes recognition of their individuality, rights and preferences, and ensuring they are at the centre of what we do and the decisions we take as healthcare professionals.
People’s voices matter. The challenge is this: how can we ensure that those voices are sought, heard, and reflected in our decisions and actions?
This report is a response to that challenge. It reflects the actual lived experience of people approaching the end of their life and those who care for them. Their experiences tell us that we have to do more – individually and systemically – to improve the experience of dying in the UK.
If we want real change, we need to find a way to evolve advance care planning, moving from broad conversations, to a place where people are supported to understand exactly how their values and priorities can inform decisions about their end-of-life care. People need to know how to document or record their wishes, and how that can help. Healthcare professionals should be supported to understand the law and guidance, and to feel comfortable following it. The healthcare system needs to change to make this easier, and routine.
I am particularly struck by how it seems death, dying and advance care planning are often ‘owned’ by healthcare. But it is everyone’s responsibility to bring death into the public consciousness and to normalise planning for the end of life. Healthcare professionals should not be the gatekeepers.
Can we change the way society views death and dying, moving towards accepting it as a normal part of life, and repositioning healthcare so that it supports, rather than owns, dying and the important conversations that surround it? That is an ambitious aim. But ultimately, although there has been positive change and improvement around the experience of dying, there is much more that needs to be done.
This report is a call to action to us all – the government, the healthcare system, individual healthcare professionals, and the public – to adopt a more open and realistic approach to death and dying and thinking ahead, to help us all have the end-of-life care we would want for ourselves and the people who matter to us most.
Vinnie Nambisan, Consultant in Palliative Medicine and Trustee of Compassion in Dying
For over a decade, Compassion in Dying’s information line has been supporting people to make decisions about their end-of-life care by planning for decisions in the future or balancing treatments with their priorities right now. This report amplifies the voices of the people supported over a two year period, from July 2021 to June 2023.
Introduction and summary
The medical options now available to people in the last years of life were unimaginable 50 years ago. In the UK, more people are living longer than ever before. The benefits of medical progress and innovation are transformative but there is an unintended consequence.
For many, it means their death is prolonged. For some dying people this is a choice that reflects their preferences. For others, it reflects a medical culture that prioritises extending life over allowing individuals to make an informed decision about whether they want this.
For those who are approaching the end of their lives, understanding what lies ahead is fundamental to their quality of life in those final months and weeks. The vast majority of people want to know the benefits of treatment, as well as the options for refusing it, and want an honest conversation with their doctor about both1. Or they may want their family and friends to be listened to if they can’t speak for themselves. If they have put an end-of-life plan in place, they expect it to be respected.
Healthcare professionals strive to do the best for their patients. This report shows though that for many dying people, their hopes of a good death – as they define it – can too often be frustrated by a medical culture and healthcare system where the default is an unquestioning approach of keeping people alive. This leads to people’s wishes being dismissed or not sought at all, the law ignored and medical guidance overlooked.
There is rightly much talk of insufficient resource in healthcare, with a great many people unable to access the treatment they need. This has a massive impact on their lives and must be addressed. However, people at the end of their lives often tell us a different story. A story of unwanted treatments, ambulance rides they wanted to avoid, and hospitalisations they said they did not want. If we want to build a modern, safe, and compassionate healthcare service that meets people’s needs and creates value for people at the end of their lives, we need to listen much harder to what people say they do not want, as well as what they do.
One in four people say the last close friend or family member they know who died received medical treatment they would not have wanted2. This should be a wake up call to everyone with a part to play in ensuring high quality end-of-life care, from policy makers to individual healthcare professionals.
This report shines a light on inappropriate over-treatment at the end of life, how opportunities to understand people’s priorities and respect their decisions are missed, and the harm this causes to dying people and those who love them. It also shows what good practice looks like and the difference this can make to a person’s death. We hope it starts an important conversation about why the experience of dying is too often made worse than it needs to be, and how we can work together to allow people to make their own informed decisions.
Current law, policy and guidance already emphasise the importance of supporting people to make their own decisions and respecting their autonomy. However, the experiences of the people we support tell us that the gap between policy and practice is often too wide and the switch from active treatment to comfort care – “from treating to caring” as one doctor put it – is an uncomfortable transition for many clinicians. To address this, we set out fundamental and achievable recommendations to change the way we approach dying in the UK.
Summary findings
Many people speak of having to “fight” a medical system that tries to extend life without considering what’s right for each person. By the time people find Compassion in Dying many are already in urgent need of support. While what we hear may not be representative of those who have more straightforward end-of-life experiences, the four themes identified here appear consistently and repeatedly for our callers:
1 – Talking about dying is not enough to ensure people’s wishes are followed
Family and friends of someone not able to make their own decisions frequently tell us that when their loved one’s wishes for end-of-life treatment are not recorded, they receive treatment they would not want. Despite the person having discussed their wishes at length previously, family and friends find themselves shut out of decisions particularly when expressing their loved one’s desire to withdraw or withhold a life-sustaining treatment. They report lasting trauma and guilt at witnessing unnecessary treatments that do not align with the person’s values and regret at not having known that recording such wishes was important.
2 – Opportunities to help people consider, discuss and record their preferences are missed
When people broach the topic of refusing treatment or advance care planning with a healthcare professional, some are stonewalled, told not to bother, or have their emotional state or mental capacity questioned. Avoiding discussing a person’s end-of-life wishes means people’s decisions may not be known or documented, and therefore are less likely to be followed if they lose capacity in the future. It means important opportunities to support them are missed. It can erode trust in healthcare professionals and leave people feeling powerless over decisions about their care.
3 – The healthcare system can be dismissive of people’s attempts to make decisions:
Advance decisions to refuse treatment are not always respected
Health attorneys are not always listened to
When people lose capacity to make treatment decisions, clinicians can be unwilling, unable or unsure how to faithfully follow through on their patients’ recorded wishes. People tell us frequently that legally-binding advance decisions are ignored or health attorneys are shut out of decisions. This causes anxiety and a sense of helplessness at an already stressful time, often resulting in a person being over-treated against their wishes, sometimes unlawfully, despite their careful planning.
4 – People cannot make informed decisions without realistic and straightforward information
Some people are not told they are dying even when they ask. Others are told critical information about their treatment options or prognosis in euphemisms or with terminology they do not understand. This can mean their understanding of a situation is very different from reality. It takes decisions out of the person’s hands and stops them from being able to make an informed choice about their own treatment and care.
A new approach
Good medical practice happens every day and in every setting across the UK. Within an increasingly constrained working environment, healthcare professionals continually do their utmost for the people under their care. The experiences of the people we support show clearly, however, that the culture around dying in the UK urgently needs a rethink.
It is a privilege to know, record and respect my patients’ end-of-life-care wishes. We have all the means to make this happen, we just need to use them. While there can sometimes be challenges and bumps in the road, walking alongside my patients on their journey, and respecting their preferences is what it means to be a good doctor.
Mark Taubert, Consultant in Palliative Medicine
Addressing the findings in this report requires culture change both in healthcare and in society as a whole. Within society, end-of-life conversations should be a normal part of life, there should be many opportunities to have, revisit and record such discussions. Within healthcare, conversations about end-of-life wishes need to start earlier and be routine. We also need a culture where clinicians are comfortable making the transition from active treatment to comfort care when appropriate, and feel confident in doing so.
These two shifts – in society and in healthcare – would reinforce each other. A more informed public that considers advance care planning as normal as writing a will, would foster an expectation of clinicians to be willing and ready to talk about death and dying. In turn, clinicians proactively initiating discussions about end-of-life wishes more regularly would help people to see this process as a normal part of healthcare, and give them ample opportunities to participate in these discussions if they want to.
England’s chief medical officer, Chris Whitty, recently called for a similar cultural shift in healthcare, away from maximising lifespan and towards improving quality of life in old age. He argues that sometimes this means “less medicine, not more” and that the key question should always be “what do people want themselves?” 3.
Ultimately, enabling people to make their own informed decisions and having those choices respected, holds the key to improving dying in this country. Everyone has a stake in this conversation. It is entirely possible to change how we die.
Recommendations summary
We are calling for collaboration from government, health and voluntary and community organisations to:
Introduce an advance care planning conversation guarantee, initially through the NHS health check
Deliver a public health campaign on advance care planning
Create more opportunities for people to record what matters to them at the end of their lives
Introduce a duty of openness and transparency in end-of-life conversations to enable properly informed consent around treatment decisions
Develop mandatory training for healthcare professionals on end-of-life decision making under mental capacity legislation
Develop mandatory training for healthcare professionals to recognise when a person is approaching the end of their life and to support a transition to comfort care
Methodology
This report contains a thematic analysis of 2,614 calls and 3,063 emails we received on Compassion in Dying’s information line between July 2021 and June 2023. The commentary and quotes used throughout the findings are taken from this analysis. The people in our case study sections have been supported by the service since 2020.
All polling figures, unless otherwise stated, are from a YouGov Plc. poll. The total sample size was 2,093 adults. Fieldwork was undertaken between 1st – 3rd March 2024. The survey was carried out online. The figures have been weighted and are representative of all GB adults (aged 18+). This report also uses data from Compassion in Dying’s service monitoring, which combines quarterly feedback from the people we support and online surveys about the experiences people are facing.
The data at the start of each finding is taken from a service monitoring survey conducted in February 2024 with 605 respondents.
The voices in this report
Our nurse-led information line supports thousands of people each year. The service is free of cost and free from judgement. We listen and offer honest and compassionate information and support, led by people’s needs. We help people make advance decisions (living wills), so their wishes are known and can be respected. And we enable dying people to get the right care and support in place when they need it.
Demand for the service has risen significantly. The number of contacts in 2023 (4,007) was a 48% increase compared to the previous year. This growth is set against a backdrop of enquiries which continue to increase in length and complexity. The proportion of our calls that took longer than 15 minutes increased by 35% from 2022 to 2023.
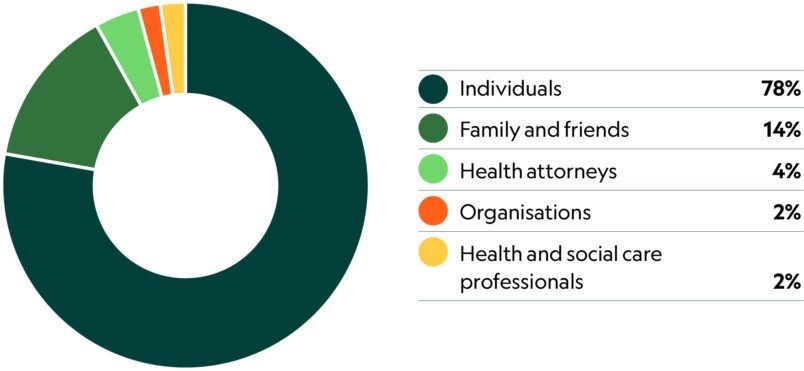
Who contacts us
75% are female
25% are male
18% have a disability
97% describe their ethnicity as white
88% are over 60
As a result of contacting the information line
88% of people felt better informed about their end-of-life rights and choices
95% of people felt piece of mind after planning ahead
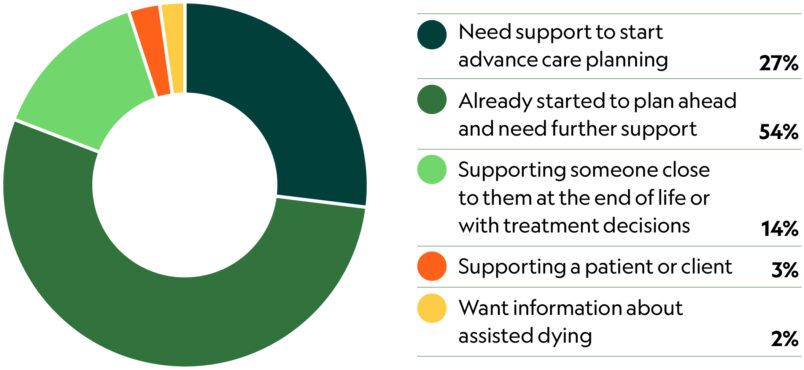
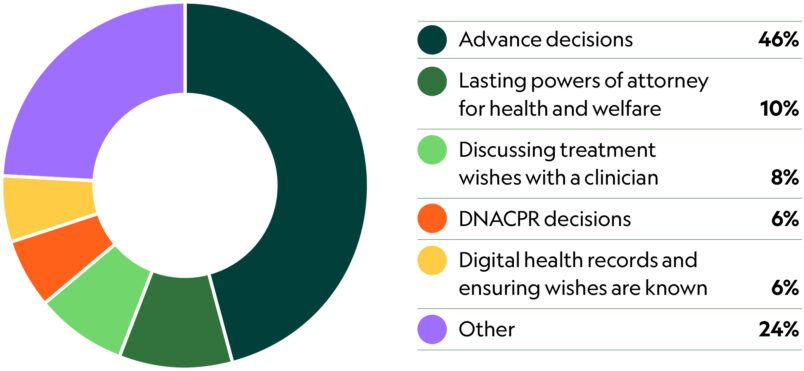
Why people get in touch
Main topic per call
Ethnic diversity and health inequity
We recognise that the people who call Compassion in Dying for support are not representative of the ethnic diversity of the UK as a whole.
Furthermore we know that advance care planning is a privilege too often unavailable to those who do not have the time or resources to proactively seek it out whilst struggling to have other basic day-today needs met, as is the case for a growing number of people in the UK.
Over the last decade, Compassion in Dying has worked with communities we know are underrepresented in our services, partnering with a wide range of local organisations to provide information and support. Often, the people we speak to through this work tell us they are very unused to feeling like they have a ‘choice’ in health matters because getting basic information or support that is both accessible and language-appropriate is such a struggle. Considering your future wishes after a lifetime of struggling to access services you need right now, for many does not make sense.
Our work with South Asian Elders4 and the wider community in Newham5 showed that people who are singly or multiply marginalised, either as a result of practical barriers like language or systemic barriers like racism, are less likely to ask questions or articulate what matters to them unless directly prompted.
By contrast, many of the people that we support through our information line have access to financial and professional resources or high levels of health literacy. Despite this, even they struggle to ensure their or their loved one’s voices are respected at the end of their lives and report feeling lost fighting a system that will not listen.
Many of the stories in this report are the end-of-life experiences of people with significant advantages. We must also consider and address how those who experience multiple disadvantage will likely struggle even more.
Inequity in experience and outcomes at the end of life is well recognised. It exists across multiple domains and systems of care6. Action across research, practice and policy is urgently needed to understand the causes of inequity, how they intersect, their impact, and how they may be redressed.
Polling: what the public thinks
83% want to prioritise their quality of life over living longer in the last years of their life
26% said the last close friend or family member they know who died received medical treatment they would not have wanted towards the end of their life*
*asked to 1,214 people in the sample whose last close friend or family member to die died of a short or long-term illness
If they had an illness like dementia or were in a coma:
90%
would want to make the final decisions about medical treatment themselves (having written out decisions in advance), or would want a friend or family member to make those decisions
3%
would want a doctor to make the final decisions about what medical treatment they were given
People told us that if they were approaching the end of life:
79%
would want a doctor to tell them if they were dying and how long they may have left to live
92%
would want a doctor to tell them the pros and cons of different treatments
83%
would want a doctor to tell them about the option of refusing life-sustaining treatment (eg, cardiopulmonary resuscitation)
85%
would want their doctor to talk to them about how to record their wishes for future care and treatment
9% of people have made a lasting power of attorney for health and welfare
5% of people have an advance decision (living will)
Findings
1. Talking about dying is not enough to ensure people’s wishes are followed
29% When caring for a dying friend or family member who had not recorded their wishes in advance, one in four people (29%) told us that they were not given an opportunity to contribute to the decision making process.
Both academic research7 and learning from Compassion in Dying’s information line, has consistently shown that if people are able to plan ahead for the end of life, and are supported to do so, it can help them to have peace of mind in the present, reduces unwanted medical interventions and unnecessary hospital admissions, and improves relationships and communication between families and healthcare professionals. The Mental Capacity Act 2005 provides valuable tools to facilitate advance care planning through advance decisions and lasting powers of attorney (LPAs) for health and welfare.
However, polling shows that while only 3% of people would want a doctor to make the final decisions about what medical treatment they were given, only 5% have completed an advance decision and 9% an LPA for health and welfare8.
My husband died while in a care home. I had made it clear that he had not wanted to have his life extended – wishes he voiced to me when his dementia was at an early stage. It did mean a great deal that his wishes were understood and followed. I was updated daily on his condition and felt involved in his care. I believe he had a peaceful ending and I was very grateful for their care.
Family members and friends tell us that when their loved one’s wishes for end-of-life treatment are not recorded, they can receive treatment they would not want. Despite their loved one telling them what they do or do not want in such situations, simply knowing and explaining this to the person’s clinician is not enough to ensure their wishes are upheld.
What the law and guidance says
The law states that if someone lacks capacity to make a decision, that decision needs to be made by someone else. Unless they have made an advance decision or lasting power of attorney for health and welfare, decision making power and responsibility falls to professionals. Whoever is making the decision must act in the person’s best interests.
The Mental Capacity Act 2005, the Adults with Incapacity (Scotland) Act 2000 and the Mental Capacity Act (Northern Ireland) 2016 provide the framework for how a person’s best interests or benefits should be identified. The law states that the person’s past and present wishes, feelings, beliefs and values must inform the decision-making process, and the views of other people who are close to the person who lacks capacity should be considered. The British Medical Association guidance9 on best interests decision making states that those close to the person must be consulted as part of the process.
Despite the best efforts to engage in their loved one’s treatment and care decisions, family and friends are often not invited to participate meaningfully in these decisions. When not listened to, people tell us they feel guilty that they are not able to successfully advocate for the person they care deeply about. They report distress that they feel could have been avoided if a proper best interests process had been followed or if they had known that such decisions could be recorded in a legally binding way. In addition, many experience lasting trauma at witnessing unnecessary treatments that do not align with the person’s values.
Experiences of trying to advocate for a loved one show clearly that even someone who understands the law can struggle to be included in the best interests process. Often the process is not followed correctly for a variety of reasons, which include pressures on time, knowledge levels, training and the efficiency of best interests processes.
“My father was in intensive care for 3 weeks before dying. The nursing staff were brilliant but the doctors disagreed and refused to accept our word about what my father would have wished. His misery was prolonged as a result. Their insistence that they could still save his life, regardless of its subsequent quality which would have been grim, seemed to trump what we knew about his strongly held beliefs.”
“My aunt lived over 100 miles away and her wishes were known to the family and told to healthcare professionals but despite this, active treatment was given following a very significant stroke aged 91 years. This led to her surviving a further 3 years with no quality of life. There was a very old handwritten note that set out her wishes, which was found after the nasogastric tube had been inserted. But it was disregarded by the health professionals. They wouldn’t involve us and didn’t ask for what we knew about her wishes.”
“Mum was 83 and was taken into hospital with sepsis due to a failed knee replacement. She was on a morphine driver and in and out of consciousness. The doctor came in and said he was going to remove her leg but mum had previously refused an amputation and so I knew she wouldn’t want this. I told them and said I didn’t give permission but was told I had no say in it and they wheeled her to theatre. I feel as though all our wishes were ignored. I wasn’t prepared for the lack of control I had over decisions.”
Jill’s mum Eva and dad Brendan
Brendan’s story (told by his daughter Jill)
My dad, Brendan, was fiercely independent and strong. He worked in the NHS for 30 years, he truly believed in its values. He died in 2023, but after suffering a stroke, we were forced to fight for seven years to try to stop him being given life-sustaining treatment.
For our family, death has always been a normal part of life. We don’t fear it and dad certainly didn’t. He talked about his views often and feared losing his independence and not being himself anymore. Years before his stroke he went to a solicitor to get an advance decision and a lasting power of attorney, but the solicitor didn’t know what to do and dad never went back. This meant he never recorded his wishes. He thought that by telling doctors himself what he wanted, that would be enough.
After his stroke he was only able to communicate for around two weeks, in this time he expressed a wish to be allowed to die. He started to refuse food and drink and although in the beginning his medical team were certain he had capacity to make this decision, once the hospital’s legal team got involved this changed. So, against his wishes, they started life-sustaining treatment in the form of a naso-gastric tube.
For the next seven years dad was a body that laid in bed and stared at me. To see him like this felt just wrong. I knew this was the opposite of what he wanted so I began fighting for dad’s wishes to be heard.
We had multiple meetings with healthcare professionals that began in July 2016, where I told them this is not the situation my dad would have wanted. Because we disagreed with the treatment the doctors were providing, they took the case to the Court of Protection, but even this took four years. With each new meeting or treatment decision that arose I had to fight for and justify what I knew he would want, but no one listened to me. They needed to listen to the people that knew him all his life, we knew dad’s wishes better than anyone but we were dismissed. They don’t know his favourite colour, his history, why he doesn’t like mashed potatoes, but I do. How can they possibly know what he wanted medically? It was like the 73 years he lived before the stroke suddenly didn’t matter anymore.
I had to fight for him because he couldn’t speak for himself. I felt like a criminal and I was treated like an evil daughter who wanted her dad to die. No one understands what it’s like trying to convince multiple people that your dad is better off dead, but in my heart I wanted him to live forever.
When I found Compassion in Dying I was feeling like I was on the edge of a cliff but thank goodness I rang. Until that point I could find no advocacy, no support and nobody to help. It’s so hard to question medical decision making.
2. Opportunities to help people consider, discuss and record their preferences are missed
57% of our callers said they have raised the topic of refusing treatment with a doctor. 16% of them then said that when doing so they felt that their wishes were dismissed or insensitively questioned.
Many people carefully consider their wishes for care and treatment as they approach the end of their lives. Polling shows that 8 in 10 people (83%) want to prioritise their quality of life over living longer in the last years of their life10. People often need support from a healthcare professional to think through these preferences or make sure these wishes are recorded and visible to those who need to see it.
My mother had several conversations with her GP about her wish to not be given life-sustaining treatments in the months preceding her death. The GP and the hospice team were excellent and fully aware and supportive of her wishes. Being reassured by them that they knew about and would respect her wishes was a source of comfort to her and us at a very sad and difficult time.
The people we support tell us that when such a conversation is open, human and non-judgemental it builds trust in the healthcare system, gives peace of mind and reduces anxiety. They feel relief at being able to discuss their end-of-life wishes with someone who is open to the conversation.
What the law and guidance says
The importance of honest discussions and the opportunity to plan for the end of life have long been recognised by key policy documents such as the Ambitions framework for palliative and end-of-life care11, the Universal Principles for Advance Care Planning12, and the NHS priorities for end-of-life care13. The Lancet Commission on the Value of Death14 recommended that national programmes should be initiated to ensure that everyone has the opportunity to make an advance care plan.
These policies have been supported by academic research which has consistently shown that advance care planning ensures individualised care, increases the use of palliative care and improves the bereavement experience.
People regularly tell us that when they try to have a conversation about refusing or stopping treatment with a clinician – now or in the future – it is closed down or discouraged.
Some people are told that they are too young or too healthy to think about these things. Worryingly, some people report that when they discuss their wish to refuse treatments it unfairly brings into question their emotional state or capacity to make those decisions. This type of response can result in a breakdown of trust between an individual and the healthcare system, leaving people feeling powerless over their decisions and that they are difficult for being pragmatic and realistic about their goals for care.
Another consequence of the reluctance to talk about end-of-life treatment is that an individual’s decisions may not be known or documented, and therefore are less likely to be followed if they lose capacity in the future. Ultimately, avoiding discussing a person’s wishes means that important opportunities to support them are missed.
“I am housebound, suffer prolapses, am incontinent and experience chronic pain. I’m managing but wanted a DNACPR form because my quality of life is already not great – the GP responded by asking if I was suicidal and said he felt very uncomfortable about being asked by someone so young. I’m pragmatic and realistic about my situation and I’m so frustrated by their response. It’s insulting and now I feel I can’t work with him to make a plan for if my conditions get worse.”
“I tried to talk about an advance decision (to refuse treatment) but the doctor thought I was only doing one because I was having an emotional reaction to my wife dying. It was very patronising.”
“I’d really like to speak to a doctor about refusing CPR. I’m 84, no terminal illness but I do have conditions that I have regular contact with a GP about. Twice I’ve asked about refusing CPR and, from two separate doctors, their response has been ‘let’s talk about that next time’. The receptionist says it’s not an urgent thing and doesn’t warrant an appointment. I’m going round in circles and just need a way in. The way I see it is this is causing me anxiety, which exacerbates my conditions.”
“When I saw a GP in March she was not willing to either: complete a Do Not Resuscitate Form or support my completing an advance decision form. In her opinion, whilst I am 85 now, she considered such arrangements to be premature on account of my general state of good health.”
Our quarterly service monitoring suggests that practice is improving in this area. In 2020, 57% of people who discussed their advance decision with their GP or healthcare professional reported a positive experience. In 2023, this number increased to 67%. But the fact that these themes are consistent and recurring shows that the culture of discussing end-of-life treatment needs attention.
“I spoke to one of my oncology colleagues. He had wanted to talk about end of life care preferences with one of his very poorly patients, but on that day, in his clinic, he’d already given the patient and his family three consecutive bits of bad news about worsening scans. He felt that talking about the end of life would have been too much after delivering so much bad news. I suggested that sometimes we have to move such discussions over several consultations, and I sometimes pre-warn the patient and their family that I may bring up the topic in my next clinic, of what we might need to think about when things are less good. I think people appreciate a warning shot, and then they can go into the consultation knowing that it will be discussed. And some then find that a very positive discussion, when it has been held.” Mark Taubert, Consultant in Palliative Medicine
Helen
Beryl’s story (told by family friend Helen)
My Auntie Beryl was a very active 73 year old. She had been a wonderful cook all her life and food was of great importance to her.
She had a brain tumour that was operated on, but the operation left her with a swallowing disorder that meant she couldn’t eat or drink. She was fitted with a Percutaneous Endoscopic Gastrostomy (PEG) feed which was very cruel for Beryl as her life revolved around her food. She started to get progressively worse over the last six months of her life and kept saying this isn’t living, I’m just existing and I don’t want to do this forever.
Beryl began to refuse her PEG feed and she was adamant in her decision. She wanted to have the right support in place so we called her GP practice to discuss her decision. Instead of listening to her they rang the mental health team and this began a huge snowball that we couldn’t stop.
Whilst Beryl continued to refuse her PEG, the next week was full of doctors and a psychiatrist visiting constantly. The first time they came they all agreed she had capacity to make this decision and was not depressed. The next day they decided the opposite and that Beryl should be taken to hospital immediately to reinstate the PEG feeding. As her power of attorney I adamantly refused.
Beryl had been declining the whole week. The palliative care team who supported Beryl’s decision were working to manage her symptoms and kept telling the visiting doctors that she wasn’t the lady they assessed at the start of the week. She was weak and she was dying. However, at midnight the next day the police, paramedics and social workers arrived to take the dying 73 year old to a high security mental health hospital. They told me that being power of attorney didn’t matter as they were sectioning her.
They were not equipped to look after Beryl at the hospital. They never tried to reinstate the PEG feed, I couldn’t understand what they were doing keeping her there. Finally she was allowed home, the palliative care team came out again, a syringe driver was fitted and she died three days later.
Her wish to refuse treatment was so hard for the doctors to hear. No one wanted to put their head about the parapet and explain how they could support her to do this. As Beryl’s closest family the whole experience was very traumatic.
3. The healthcare system can be dismissive of people’s attempts to make decisions
Polling shows that if people had an illness like dementia or were in a coma, 9 in 10 would want to make the final decisions about medical treatment themselves (having written out decisions in advance), or would want a friend or family member to make those decisions15.
The tools that exist to enable people to make decisions in this way, namely advance decisions and lasting powers of attorney for health and welfare (LPAs), are therefore incredibly valuable and more people need to be made aware of their existence. When people’s right to make decisions is treated as paramount and their wishes recognised and respected, the impact is profound. People feel listened to, valued and more in control. Healthcare professionals can feel reassured that they have given care which aligns with the person’s vales and wishes. The right documentation can ensure a person’s treatment is appropriate, they are not given life-sustaining treatments they do not want, and family members are listened to and valued.
Too often though, even when such planning is in place, these crucial documents are not followed. The experiences of the people we support show that this is particularly the case when doctors disagree with the decisions being made. People tell us frequently that legally binding advance decisions are ignored or health attorneys are dismissed, causing anxiety and a sense of helplessness at an already stressful time.
Advance decisions to refuse treatment are not always respected
18% of people who supported someone at the end of their life who had an advance decision or DNACPR decision report having had to fight to ensure the document was respected.
When a person wishes to refuse treatment, an advance decision or Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) decision can be instrumental in ensuring someone’s wishes are known and respected.
“When my husband’s heart condition suddenly declined he ended up under the care of a different doctor, who didn’t really know him. He attempted to admit my husband to hospital and force treatment on him that I knew he didn’t want. It was very frightening for both of us to face such insistence but, thanks to the advance decision and lasting power of attorney, I had evidence of my husband’s wishes and, only because of that, the doctor listened. It ensured my husband’s wishes were followed. I really felt I was being bullied and losing ground and I don’t believe that I could have advocated for what he wanted without those documents.”
Although most of the people we support tell us that having an advance decision in place helps to ensure that treatment is appropriate and aligned with the person’s wishes, it is important to address the fact that a steady proportion of people find these legal documents are ignored when a decision about life-sustaining treatment needs to be made.
What the law and guidance says
Anyone over the age of 18 with mental capacity can write down specific treatments, including life-sustaining treatments, they wish to refuse in an advance decision in case they become unable to make or communicate those decisions in the future. A valid and applicable advance decision to refuse treatment is legally binding in England, Wales16 and Northern Ireland17. In Scotland18, national focus on anticipatory care planning includes information for healthcare professionals and the general public on how these forms must be taken into account when deciding on how to treat the person.
There are clear policies regarding the refusal and/or the withholding of cardiopulmonary resuscitation (CPR), an important component of advance care planning. Guidance from the British Medical Association, Resuscitation Council UK, the Royal College of Nursing19 and the NHS20 show how these decisions, once made, should be communicated and followed.
This means basic principles of autonomy are not upheld and people receive treatments they do not want. It results in a person’s death being needlessly drawn out and them having to endure a situation in their final weeks and months that they tried hard to avoid.
For loved ones, the impact of witnessing somebody’s wishes being overlooked causes distress at a time when they are already facing profound grief.
People also tell us they are made to feel guilty for trying to implement their loved ones’ wishes and are subsequently shut out of decision making conversations with the healthcare team. This leaves people feeling alienated from their loved one’s care and unable to trust the healthcare system to respond to their loved one’s individual needs.
“My husband was diagnosed with Alzheimer’s at 52 and died around 8 years later. I looked after him for 6 years and then when I could no longer manage he moved to a care home. He spent the final two years almost always screaming. Despite having an advance decision in place that refused life-sustaining treatment, he was routinely given antibiotics for life-threatening chest infections without any consideration of alternatives. It was such needless suffering.”
“My lovely mum died in hospital. Despite having a DNACPR form in place, when she had a cardiac arrest, she was given CPR. It took the team around 10 minutes to revive her. She was intubated and we were advised that the prognosis wasn’t good and she would likely die within two hours. She was unconscious and experiencing agitation and distress. In the end the tube was removed and my mum died within a couple of minutes. To know she went through such stress unnecessarily at the end is very upsetting and distressing.”
“My gran died from vascular dementia aged 101. Until her mid 90s she was strong, healthy, active, independent, but deteriorated slowly and painfully, losing her independence and hating every minute of it. She had made an advance decision, with support from her GP and us. Doctors at the local hospital totally ignored her refusals of life prolonging treatment and she received treatment she had refused. One doctor said to me they never took any notice of them.”
Natalie looking at Anne’s advance decision and DNACPR forms
Anne’s story (told by her daughter Natalie)
Before my mum, Anne, was diagnosed with Alzheimer’s she was vibrant. She was highly intelligent and full of life. She never feared death and brought the whole family up to share her pragmatism and we talked about death often.
Long before her diagnosis, she wrote a DNACPR form with her doctor; she put a health power of attorney in place; she wrote an advance statement with her health preferences and an advance decision to refuse treatment. Her advance decision refused all life-sustaining treatment if she lost the capacity to make this decision for herself. She was the type of person who thought everything through thoroughly and felt strongly about her views; she even had DNAR tattooed across her chest. She begged me “If I can’t speak for myself please fight for me”. I promised her I would.
She moved into a care home at the start of last year, but it took me several months to realise that her care plan had no record of any of her prior planning or carefully considered treatment decisions. I was shocked when I read that she should be resuscitated. Someone had clearly written that my mum had not expressed any end-of-life wishes and that it would be discussed “when the time comes”. It was frightening. If something had happened to her prior to this moment all of her planning might as well have not existed.
I continuously chased the care home staff but they just weren’t used to dealing with someone who had strong feelings about their end-of-life wishes. I’m convinced that her refusal of treatment and acceptance of death was much harder for them to deal with than if her documents said ‘keep me alive’.
Finally, after months of work, her documents were taken on board by the senior care home staff but I didn’t feel confident they were understood by anyone. They would ask me strange questions like should they just leave her and not do anything if she had a fall. But in fact mum’s advance decision didn’t refuse all treatment, it just refused life-sustaining treatments, there is a big difference and I was terrified that the people caring for her didn’t understand this.
The thing that worries me is if mum didn’t have me to fight for her to get these documents accepted and understood, what would happen? This has been a frightening year and throughout I felt so lost in trying to fight for her wishes. There is no one out there you can go to for help, Compassion in Dying were the only people I could find who would. If they hadn’t picked up the phone and talked me through the law and what I should expect from her care I just wouldn’t have been able to push for her wishes.
Health attorneys are not always listened to
35% of the people we support said they have acted as a health attorney for someone close to them. 14% of them then said that they felt ignored and excluded from decisions about that person’s care when trying to act as an attorney.
People who have trusted friends and family around them can appoint a health attorney to make decisions for them if they cannot make decisions for themselves, instead of leaving these decisions to health and social care professionals. People tell us that making an LPA gives them peace of mind, and many feel reassured about the legal weight it should, in principle, hold.
“My wife had cancer and as her health declined during the final days, she was moved from hospital to a hospice. We had previously had conversations about how things should be at this point; having the LPA in place meant that I was able to work closely with the doctors and staff to help manage things like medication and care levels when she couldn’t make those decisions herself. Despite all the things that were happening to her, she was still able to smile and laugh until the final moments as we were getting things right for her.”
Despite the legal decision making power an LPA gives, health attorneys tell us consistently that their opinions are dismissed when trying to make decisions for someone they love.
What the law and guidance says
The legal status of a lasting power of attorney recognises the value people place on enabling those they trust to make decisions on their behalf. The right to give legal authority to someone they trust to make treatment and care decisions on their behalf when they are no longer able to is set out in the Mental Capacity Act 2005 and in the Adults with Incapacity (Scotland) Act 2000. An appointed ‘attorney’ has legal authority to make health and care decisions and has a duty to make those decisions in the person’s best interests.
Health attorneys often know their loved one best and are trusted implicitly to make these decisions if the time comes to do so. However, they are shut out of decisions even when they can explain, with evidence of previously expressed wishes, why the decision in question is in their loved one’s best interests. Almost exclusively, people tell us that these experiences occur when health attorneys are concerned their loved one is being over-treated and try to refuse treatment on their behalf.
Health attorneys can then lose confidence and feel unable to speak up further. People report feeling at a loss for how to protect their loved one from over-treatment, and feel like their motives are questioned because they try to stand up for what the person would have wanted.
“My husband has lost capacity and is living in a care home. I am his health attorney. We recently had a best interest meeting with the care home because they have refused to stop antibiotics for life-threatening infections. The manager said to me ‘if someone was drowning in a pool you would try and give them air’. I am really upset about this as I want to do what is best for him and I know he wouldn’t want to live like this. I’m worried I’ll get accused of manslaughter if I keep insisting they stop giving him antibiotics and just keep him comfortable.”
“I am an attorney for my aunt who has advanced Alzheimer’s. She was admitted to hospital and had very little decision making capacity. They took her for surgery with no discussion despite knowing I was her health attorney. I repeatedly tried to give them documentation to prove this but they said they didn’t need it. They also said they will treat her and get her fit enough to get back to the home – that was their aim. I’m upset as my aunt would never have wanted this and they didn’t listen to me when I tried to explain.”
“Dad has advanced dementia and is in a care home. As we are his health attorneys I explained he wouldn’t want nutrition and hydration, but the nurse said our views didn’t matter as it was their duty to prolong life.”
“My dad is in a care home, my siblings and I have lasting power of attorney for health and welfare. GP and the care home clinical lead had a best interest meeting with us in summer and decided no more antibiotics for life-threatening infections. We were all in support and the GP recorded this on his medical record. The Care home manager today said she ‘can and will’ override this decision or dad cannot remain in the home.”
Chris
Dione’s story (told by her son Chris)
For more than two decades before she died, my mum, Dione, had repeatedly asked me to make sure that she would be allowed to die when she was ready to go. I made her that promise. She had a DNACPR form from her doctor, she appointed me as her health attorney through an LPA for health and welfare and had an advance decision to refuse treatment. Her advance decision included a refusal of all life-sustaining treatment if she were to suffer from a stroke.
In November 2021 my mum had a stroke and was moved into hospital, she spent the first week wanting to come home, but things moved quickly and in her second week she suffered a heart attack followed by a second stroke. We knew mum was dying, and by this point there was no doubt what her wishes were: she wanted to die naturally without having her life prolonged. She was shouting for the world to hear “let me go home and let me die”.
As her son and health attorney, it was my job to make sure the hospital respected her wishes. When I tried, my authority as her decision-maker was not taken seriously. When I tried to explain what her wishes were or show them her advance decision form both were dismissed. I wasn’t listened to and mum kept being given antibiotics for life-threatening infections that I knew went against her previously expressed wishes.
When I asked who had given consent for these treatments, none of the nurses had an answer. When I finally got to meet a registrar she admitted that there was no record of consent being sought from my mum. She clearly did not think this was important and shrugged it off. Rather I was made to feel like a nuisance. Clearly my mum was not able to give informed consent and yet I was not being consulted either. I had lasting power of attorney, I had her advance decision, it was very clear that she didn’t want her life prolonged and they should have stopped.
For two weeks I struggled with the hospital, trying to get my views heard. I didn’t know anything about how hospitals functioned. I just knew that I wasn’t able to get what I, by that stage, knew my mother wanted, which was to be allowed to die naturally.
When I was finally able to speak to the senior consultant, I had rehearsed what I wanted to say and I was ready to explain my mum’s wishes thoroughly. However, he opened that meeting by saying that he didn’t need to hear anything from me, he told me in situations like this they’d “do their best” for their patients. I was shocked. As her health attorney I was being told by the senior clinician in charge that my views didn’t count.
In the end, mercifully, my mum was moved to palliative care and I finally felt I was being treated the way I would have liked to have been from the start.
4. People cannot make informed decisions without realistic and straightforward information
51% of the people we support have told us they, or someone they have cared for at the end of life, had to make a serious treatment decision. One in four (25%) of them then said that they would have liked more information to help them make a properly informed decision.
When clinicians give realistic information, use language people can understand, and allow time and space for questions, people and their families have a better experience. Care is more likely to be person-centred and people are able to make properly informed decisions.
“My brother had kidney failure, and I’ll never forget how one consultant was always so straight up with us. Every time there was a decision to be made he was really clear saying things like ‘this is what is likely to happen if you do nothing, if you do this then it might make you feel rubbish for quite a long time’ and so on. He asked my brother every time he saw him what his next goal was in life and told him how likely that was to happen and what might help him get there. I thought that was amazing, like everything was based on my bro and what he needed to make his own decision. It was such a ray of light at really stressful moments, he just treated my brother like an intelligent human being.”
Polling shows that most people want honest and pragmatic conversations about their options and treatment. 92% of people said that if they were approaching the end of life they would want their doctor to tell them the pros and cons of different treatment options. 83% said they would want the doctor to talk about the option of refusing life-sustaining treatment24.
What the law and guidance says
The General Medical Council (GMC) guidance on decision making and consent21 requires clinicians to explore what matters to the person, so they can share information about the benefits and harms of proposed options. This should include reasonable alternatives and the option to take no action.
GMC guidance on good medical practice22 sets out overarching principles, including that clinicians should recognise that people are individuals with diverse needs; not make assumptions about the options or outcomes someone would prefer; and consider how their own life experience, culture and beliefs might influence their interactions with others or impact on their decisions and actions.
The GMC guidance on treatment and care towards the end of life23 includes that there is no absolute obligation to prolong life.
Despite clear guidance however, people often tell us they are not given realistic information about their condition or treatment options. In some situations this means medical terms and acronyms are not explained properly and sometimes euphemisms are used instead of being clear about the person’s current health and likely prognosis.
Terms commonly used in healthcare, such as ‘stage 4’, ‘palliative care’, or ‘DNACPR’ are not understood by everyone. This is especially the case for people who do not speak English fluently or need an interpreter in healthcare appointments. Furthermore, people tell us that language barriers between themselves and healthcare professionals mean conversations during appointments can be challenging. For a great many people, organising interpreters is at best not straightforward and at worst not an option.
Failing to check that someone understands the words used and the options available can mean their understanding of a situation is very different from reality. They cannot make informed decisions about their own treatment and care, although they often do not realise this at the time, and the concept of shared decision making is therefore impossible to achieve in reality.
Bereaved family members tell us that not being given honest, straightforward information about their health, prognosis or treatment options prevented their loved one from having important conversations and adequately planning for the end stage of their illness. They say that for them and the dying person, not being given an opportunity to understand that they were dying is devastating. Both dying people and bereaved people tell us that although hearing bad news would be hard in the moment, it is preferable to the impact of not being told at all. This is also a sentiment repeatedly expressed by people who do not receive proper communication about a DNACPR decision that has been made.
“One doctor said to me “man to man, if I were you I’d go and make the most of your time now. If you want a drink, have a drink”. At the time I thought that’s nice, but then it dawned on me that he meant my kidney failure was end stage. I know now that I only have a few weeks left, but only because I asked ten times. It was like I had to give him permission to be honest but I don’t think that’s fair on me to know to do that.”
“My uncle had advanced heart failure, having seen the notes now it was said to be end stage/ for palliative care, but no one ever told me. He died a few days later. In hindsight having read all the notes, a discussion needed to take place, if I had known we would have looked after him at home and made plans together.”
“Well, what would happen is we would go to appointments and then the doctor would just do the routine checks and check her blood. On one occasion they mentioned palliative care, and I didn’t even know what the meaning of the word was during the meeting. Part of me didn’t want to know. Sitting there and nodding away, thinking that maybe that’s the next step to her getting better.”
“I never fully understood what healthcare professionals meant when they used words like palliative care and DNACPR while my friend was dying. It was only after he died that I finally googled them. I wish I had known, I could have talked to him and found out what he did and didn’t want.”
Photos of Alan and Sonya
Alan’s story (told by his wife Sonya)
I was married to Alan for almost 29 years, he was diagnosed with stage 4 lung cancer and died 6 months later. We were never told that his condition was terminal.
We were told it was stage 4 lung cancer and were expected to know what this meant, but this was our first experience of dealing with anyone with cancer so we were completely in the dark. Alan said to the oncologist “I am very relieved because I thought I was coming in here today for you to tell me to get my affairs in order” but nobody challenged this.
Alan was under the assumption that his condition was not terminal and with chemotherapy, he could come out the other side of this. Alan began undergoing gruelling chemotherapy. If he’d known his condition was terminal he would never have put himself through this.
Alan then suffered a saddle pulmonary embolism and was hospitalised. Whilst in the hospital I got a phone call from the nurse on the ward, she told me they now believed Alan was in the terminal phase of his illness. This was the first time we had heard that word. He was discharged with a syringe driver, a hospital bed and district nurses coming in each day.
Every time healthcare professionals came to the house I would ask them– does he have long? But nobody would tell me. I know it may not be something people can approximate, but there must be signs that someone is dying. I wasn’t told any of them.
A few days later Alan’s breathing got strange. So I phoned the district nurses and said his breathing is different, what do I do? All they said was to hold his hand and talk to him. No one told me what was happening and no one came out to help. Alan died that day. I didn’t know he was taking his last breaths, we weren’t prepared and no one told me he was dying.
After Alan had died I raised this issue as to why the words terminal or life limiting were never used to us. The hospital responded to say the consultant didn’t tell patients they were terminal unless they specifically asked. For a lay person like us, how do we know what questions to ask? We rely on doctors, consultants, healthcare professionals to guide us and we rely on their expertise. But that never came across.
What I would like to come out of this is honesty and proper communication, because not having this robbed Alan and his family the right to plan how he wanted to live with his diagnosis. It also robbed us of the ability plan how he died. We had no support and I live with this guilt. We should have been allowed to make informed decisions but that didn’t happen.
Recommendations
Addressing the findings in this report requires culture change both in healthcare and in society as a whole.
Within society, people need clear and accessible information to help them consider their priorities and understand the treatment decisions they might be faced with as they approach the end of their lives. They need to know how they can record their decisions and that it is often crucial to do so if you want your wishes to be respected. End-of-life conversations should be a normal part of life, there should be many opportunities to have, revisit and record such discussions.
Within healthcare, conversations about end-of-life wishes need to start earlier and be routine. People want to have these conversations,25 so healthcare professionals need support to feel confident facilitating such discussions with pragmatism, empathy and honesty. There needs to be a common understanding that good care both at the end of life and before, includes seeking out and valuing what the person wants. Fundamentally, people need realistic information about treatment options and many want to know if they are dying26.
We need a culture where clinicians are comfortable making the transition from active treatment to comfort care when appropriate, and feel confident in doing so. There also needs to be a common understanding that in some situations, withdrawing treatment is the most caring option.
These two shifts – in society and in healthcare – would reinforce each other. A more informed public that considers advance care planning as normal as writing a will, would foster an expectation of healthcare professionals to be willing and ready to talk about death and dying. In turn, healthcare professionals proactively initiating discussions about end-of-life wishes more regularly would help people to see this process as a normal part of healthcare, and give them ample opportunities to participate in these discussions if they want to.
There is no single solution that will achieve all of this. Cultural change requires behavioural, habitual and mental shifts, both at a community level and across the environments in which people experience healthcare. It needs consideration that spans from big ideas down to the policies and procedures that underpin them.
This report has already acknowledged that policies and clinical guidance assert the importance of allowing people to make their own decisions and respecting their autonomy. However, the gulf between what policy says and the reality for many remains too wide. It is clear that guidance alone is not enough to change culture and a more radical approach is needed.
We have therefore developed recommendations that require collaboration across government, health and Voluntary Community and Social Enterprise (VCSE) organisations. In this mission, there is a part to play for everyone. These recommendations would influence how we as a society understand and talk about our end-of-life treatment and care, and would support professionals to seek people’s end-of-life wishes routinely.
They are not exhaustive, but complement the work of many individuals and organisations who are also working to change the way people die in the UK. The Lancet Commission on the Value of Death said “the responsibility for dying well should not fall solely to health and social services, nor solely to communities; a partnership approach involving shared power, shared decision making, and co-design of services is essential to enable people to die well” and we believe that collaboration at every level is essential to achieve long-term change.
The experiences in this report show that decisions about dying and end-of-life treatment need attention from clinicians across all specialisms and across all stages of a person’s healthcare journey.
We hope these recommendations will kick-start a national conversation about how to better allow people to make their own informed decisions. It is possible to forge a more compassionate approach to dying in this country, where people’s autonomy is fostered and choices are respected.
Culture change in society
Culture change in healthcare
Accessible information provided on advance care planning earlier and throughout life
Advance care planning conversations that happen routinely
Better understanding of how to record decisions and how it can help
Providing realistic information about diagnosis and treatment options so people can make informed decisions
Advance care planning conversations expected by people as a routine part of healthcare
Having confidence to recognise when treatments are not helping someone to get better and that they are likely to die from their illness
More opportunities to record end-of-life wishes
Having confidence to move from active treatment to comfort care when appropriate
Understanding the importance of respecting people’s wishes and decisions
Recommendations summary
We are calling for collaboration from government, health and voluntary and community organisations to:
Introduce an advance care planning conversation guarantee, initially through the NHS health check
Deliver a public health campaign on advance care planning
Create more opportunities for people to record what matters to them at the end of their lives
Introduce a duty of openness and transparency in end-of-life conversations to enable properly informed consent around treatment decisions
Develop mandatory training for healthcare professionals on end-of-life decision making under mental capacity legislation
Develop mandatory training for healthcare professionals to recognise when a person is approaching the end of their life and to support a transition to comfort care
Recommendation 1
Introduce an advance care planning conversation guarantee, initially through the NHS health check
Requires collaboration from: Government, NHS England, ICBs, Royal College of General Practitioners
Discussions about future care wishes should take place before a crisis in a way that is routine rather than exceptional. These discussions should focus on what a person’s priorities and preferences for care are, or are likely to be in the future. Everyone should be given the opportunity to make an advance care plan if they want to, and should have the opportunity to revisit this as their health and life changes.
Introducing these conversations at NHS health check appointments at certain ages would help enable this. These conversations should be opt-out, rather than opt-in, to ensure that they happen, with healthcare professionals required to provide information and offer the conversation.
The guarantee should be routinely promoted via the NHS App and in the community through, for example, GP waiting rooms. Over time, people would come to expect these discussions and healthcare professionals could feel confident that they are starting an important conversation at the right time, rather than seeing it as a difficult conversation which can be uncomfortable to approach.
NHS England could run local pilots to explore at which points in a person’s life or healthcare journey these conversations work best, how to promote them in different communities and develop a body of knowledge on best practice relating to the information needed in such conversations.
VCSE organisations such as Compassion in Dying already have a wealth of knowledge in how to start advance care planning conversations and this should be built into any pilot or roll out to ensure discussions are high quality and add value for the person.
Incentivisation through the Quality and Outcomes Framework would help to ensure as many people as possible could benefit from the scheme, and encourage clinical buy-in for it. Additionally, as the NHS health check scheme only runs until people are 74 years old, opportunities to continue these conversations routinely after this age also need to be identified.
Recommendation 2
Deliver a public health campaign on advance care planning
Requires collaboration from: Government, Department for Health and Social Care (DHSC), Office for Health Improvement and Disparities, NHS England, VSCE organisations
There is a clear and worrying disconnect between the high number of people who want to make decisions about their end-of-life care and treatment, and the low number who have had an opportunity to discuss and record their wishes. Polling shows that whilst only 3% of people would want a doctor to make the final decision about end-of-life treatment, just 9% have made a lasting power of attorney for health and welfare, and only 5% have made an advance decision27.
This demonstrates the urgent need for better public information on how people can plan for the end of their lives and why doing so can help. This information should be delivered through an ongoing, public health campaign which explains:
The different ways people can plan for and make decisions about their treatment and care at the end of their lives
How and why planning can help
The sorts of decisions people might face and how their values can inform these decisions
That any decisions can and should be revisited over time
That people do not have to plan ahead if they do not want to
This campaign would complement any focus on prevention in health because it would normalise the importance and impact of planning ahead on health and quality of life. The aim would be not just to inform, but to help familiarise people and families with the language used to talk about end-of-life care and advance care planning, and bring it more fully into the public consciousness. It therefore needs a long-term approach that can evolve according to the needs of different communities and emphasise key information over time.
Such a campaign needs careful research and attention to the audience, messaging and tone. It should be co-designed with people living with serious, life-limiting illness and those with experience of end-of-life discussions, as well as those who have never engaged in such conversations. To ensure reach, it needs collective leadership and collaboration from government, healthcare providers and the VCSE sector.
Such a campaign needs careful research and attention to the audience, messaging and tone. It should be co-designed with people living with serious, life-limiting illness and those with experience of end-of-life discussions, as well as those who have never engaged in such conversations. To ensure reach, it needs collective leadership and collaboration from government, healthcare providers and the VCSE sector.
Any information should be developed in a variety of languages and formats, including video or audio, given that we know some communities, particularly those whose languages are mainly verbal, prefer to listen to and watch information rather than read written content28.
Recommendation 3
Create more opportunities for people to record what matters to them at the end of their lives
Requires collaboration from: NHS England, NHS Digital, DHSC, VSCE organisations, health and social care professionals
This report shows that for many people, knowing what their loved one wanted was not enough to ensure their wishes were upheld at the end of their life. People who have to fight for their family or friend’s decisions to be respected when they lose mental capacity, repeatedly say they wish they had known about the options for recording end-of-life wishes in advance. We therefore believe there needs to be more opportunities for people to record their preferences and decisions.
The helpful concept of ‘death literacy’ – the knowledge and skills that help people to gain access to, understand and make informed choices about the end of life – is gaining momentum thanks to organisations such as Hospice UK, Marie Curie and Sue Ryder. Any work to foster a death literate society must include informing people about a series of practical things that can help them to have the death they want. These can include making an advance decision, advance statement or lasting power of attorney, having a DNACPR form, and knowing the right questions to ask to get honest information.
Our long-term ambition is that in the future there would be a nationwide advance care planning service, commissioned and run by the NHS, building public and professional understanding of advance care planning and considering the blueprint of the Office of the Public Guardian’s lasting power of attorney service in its development.
However, acknowledging that this would take considerable time to develop and with the understanding of current spending and staffing pressures on the NHS, a medium-term and significant improvement would be for The Department for Health and Social Care and NHS England to allow people to easily complete an advance decision or advance statement through already established and well-known channels such as the NHS App and local digital care planning solutions.
Well used and rigorously tested online advance care planning services already exist, for example Compassion in Dying’s online advance decision service.
This would build trust in and increase understanding of the different ways people can record their decisions and how to do so. These recorded decisions and wishes should then be shared electronically and seamlessly with everyone involved in that person’s care29.
What Compassion in Dying is doing to help
We deliver the UK’s leading free online advance decision service
Our pioneering online advance decision service30 is the largest of its kind in the UK. It’s based on the experiences of the 45,000 people who we have supported to plan ahead online for free. We developed and tested the service in partnership with people, clinicians and legal professionals. The paper version of this online service is already white labelled by NHS Trusts, primary care networks, hospices and national charities, and is linked to by the NHS.
We also allow other organisations to white label this online service for free. This means that they can integrate it with their own website or app using their branding. We share openly because we want as many people as possible to be able to plan for the end of life. Our mission is to make sure everyone receives the information they need to be in control of their end-of-life decisions, regardless of who they turn to for support.
Recommendation 4
Introduce a duty of openness and transparency in end-of-life conversations to enable properly informed consent around treatment decisions
Requires collaboration from: NHS England, Government, Royal Colleges, Parliamentary and Health Service Ombudsman
Several initiatives have attempted to rebalance the power dynamic between healthcare professionals and patients. Ten years ago, the Duty of Candour introduced a legal duty on providers to act in an open and transparent way if mistakes have been made that impact patient safety. More recently, Martha’s Rule has meant that patients will now have a mechanism through which they can request that their care is urgently reviewed if they are not being listened to and feel something is going wrong in their treatment.
The people we support clearly ask for transparency both at the end of life and when decisions about serious medical treatment need to be made. This is essential for each person to be able to make properly informed decisions about what is right for them. When people do not want to know this information, this wish must be respected. However, the starting point in conversations should be a presumption that people need clarity and honesty.
The law is clear that a person must give their consent before any medical treatment is given31. For consent to be valid, it must be voluntary and informed. However, without realistic information a person cannot give informed consent.
A blueprint for what should be included in such conversations already exists in the General Medical Council’s Good Medical Practice guidance32; specifically that clinicians must give patients the information they want and need in a way they can understand, must encourage an open dialogue about people’s health, ask questions to allow them to express what matters to them, and respond honestly to their questions. This includes information about:
their condition, likely progression, and any uncertainties about diagnosis and prognosis
the options for treating or managing the condition, including the option to take no action
the potential benefits, risks of harm, uncertainties about, and likelihood of success for each option
In addition, to fulfil this duty clinicians must sensitively provide information, even if not prompted to do so, to explain:
clearly, without euphemism or jargon, if a person is likely to die from their condition (unless they specifically say they do not want to know)
There are several possible mechanisms for such a duty, for example through inclusion in the NHS Constitution or extending the Duty of Candour to include end-of-life conversations. However, whatever the vehicle, consideration must be given to the most effective way to embed and normalise such conversations in healthcare practice. Guidance alone will not change habit, mind-set and culture. The Parliamentary and Health Service Ombudsman would be well placed to review how well this principle is being embedded into healthcare practice over time.
Recommendation 5
Develop mandatory training for healthcare professionals on end-of-life decision making under mental capacity legislation
Requires collaboration from: Royal Colleges, Health Education England, Personalised Care Institute, VCSE organisations, people with lived experience
Every person who shared their story in this report has stressed the need for better support for healthcare professionals so that they understand people’s rights to make decisions and feel confident respecting them.
Training on end-of-life decision making when someone has and has not planned ahead should be specific to the part of the UK they are in, and include:
The legal status of advance decisions and how these should be followed in practice
A thorough understanding of the best interests decision making process, when this should be followed, and who should be involved
How to use a written record of someone’s wishes for care (such as an advance statement) to inform best interests decision making
The legal decision making rights of a health attorney
The practical application of this training in real time scenarios
Appropriate training on relevant legislation, such as the Mental Capacity Act already exists, including that available through Health Education England. What is needed is for this training to be mandatory and continuing. Compassion in Dying and other VCSE organisations have deep knowledge of what happens when these principles are not well understood, and could support the design and delivery of such training.
This training should be revisited regularly (every 2-3 years). Clinical governance should be utilised for this topic. For example, regular audits on the number and quality of end-of-life care conversations should be carried out and documented, enabling training to then be further focused to departments that need additional support.
What Compassion in Dying is doing to help
We deliver a specialist, in-depth support service for people at crisis point
People fighting for their loved ones’ wishes to be heard told us they could not find help when they needed it most. Our phone-based ‘in-depth support service’ was set up to change that. Through it we help people who feel that decisions are not being made in their loved ones’ best interests, or health attorneys who are being ignored. We give people the information and support they need to write letters, communicate with healthcare professionals, prepare for best interests meetings, and enable health attorneys to better understand their role.
“Dealing with my mum dying was a terrible shock; but to then be faced with no one caring about her wishes was traumatic. Before I found Compassion in Dying there was no one who I could talk to or contextualise what was happening. When they picked up the phone it was like somebody threw me a lifeline. They gave me the information and suggestions I needed to engage with the system as an attorney and fight for my mum’s wishes to be respected at the end of her life. Regular conversations with Compassion in Dying helped me navigate an unfriendly and confusing system and finally get the result mum would have wanted.” Chris, who was supported by the service and whose experience is shared above
Recommendation 6
Develop mandatory training for healthcare professionals to recognise when a person is approaching the end of their life and to support a transition to comfort care
Requires collaboration from: Royal Colleges, medical schools, Personalised Care Institute, VCSE organisations, people with lived experience
People’s experiences show that for some healthcare professionals considering making the transition from active treatment to comfort care only is not an easy process and they do not always feel confident in doing so. This a fundamental part of medicine and doing it appropriately and sensitively requires skills and knowledge that need to be practiced, role modelled and normalised.
Putting mandatory and ongoing education on this practice into the curriculum of medical students would help to set an expectation that this type of decision making is an essential part of good care at the end of life and would support it to happen more routinely over time. It should form an ongoing thread in the curriculum which starts in year 1 and runs through to the final year of studies. This training must also be reinforced for junior doctors to enable them to practice and develop these skills over time, and should therefore be an essential component of postgraduate medical training.
For training such as this to be successful, it needs whole teams to understand it, not just individual decision makers. Embedding this training also requires an organisational culture that demonstrably values this decision making and needs systems and processes that make this sort of decision making an easy thing to do.
It should be developed in collaboration with people with lived experience of end-of-life decisions, their families and relevant voluntary sector organisations.
This training, focussing on both theory and practice, should include:
Stories of people with lived experience
How to recognise that a person is likely to be approaching the end of life
How to discuss end-of-life treatment and care sensitively and effectively with people in different healthcare settings (e.g. at the bedside, in GP clinics)
The ethics and law around death and dying, including the obligation to respect the autonomy of the dying person, the contribution family and friends can make to realising that and shared decision making
Understanding how and when to transition from providing active, disease-modifying treatments to treatments that focus on symptom management and comfort care
Legislation and legal pathways through which people can plan for end of life, how to document end-of-life conversations and agreed treatment decisions, or how to signpost people appropriately for support to do so
What can happen if you avoid conversations about people’s end of life wishes or ignore the wishes of the person
Brinkman-Stoppelenburg A, et al, The effects of advance care planning on end-of-life care: a systematic review. Palliat. Med. 2014 Sep;28(8):1000-25 https://pubmed.ncbi.nlm.nih.gov/24651708/
This important report shows how far we have come and how much further there is to go in enabling people to have as good a death as possible. Recording our wishes is one thing, making sure they are implemented is another. This report is based on experience and expertise and shows what needs to be done. I applaud the authors for their emphasis on respect and compassion.
Lord Nigel Crisp – former Chief Executive of the English NHS
Whilst one of the purposes of a good health service is to help as many people as possible have a healthy life, it is also important for that health service to ensure that people have the kind of death that is right for them as individuals. This report shows that far too often, people’s wishes for a good death, without unwanted treatments, are ignored. Importantly it also explains what we as a society and a health service can do to change this. As a society we need to have a clear conversation about how we want to die and also much more realistic conversations between clinicians and patients.