A lack of adequate systems to share end-of-life wishes causes anxiety and poor experiences at the end of life. This report proposes an overhaul of electronic records and sets out what people need them to do.
For those of us working in health and care, whether on the front line, in the voluntary sector or in commissioning, it can be easy to think of digital systems and electronic patient records as an add-on to good care rather than central to it.
But the insights from people experiencing end-of-life decisions first-hand show clearly this is not true. People genuinely care about their electronic end-of-life care records. Many experience significant anxiety that these records will not work in the way they are intended to when it matters most.
Some have lost trust in the NHS to know about and respect their wishes and the wishes of those close to them. The experience of witnessing the recorded wishes of someone close to you not be known about, or even being ignored, can be traumatic and adds to the stress and pain of the bereavement experience.
It is my sincere hope that the new Palliative and End of Life Care Information Standard, commissioned by NHS England and published by the Professional Record Standards Body (PRSB), will address many of the concerns expressed by the people interviewed for this report. The IT systems that underpin people’s electronic records must ensure that their wishes and important health information will be known about at the end of their life.
However, the new Standard is only one piece of the puzzle. We know that even in areas with well-established electronic end-of-life records, people’s wishes were still overlooked. People need digital systems that meet their needs but they also need healthcare professionals to have conversations with them about their wishes, record them accurately, know where and how to look for someone’s advance care plan, and importantly to act upon it.
We share the experiences within this report in the hope that commissioners, leaders in health and care, clinicians and health and care staff will listen to what people told us and therefore understand how vitally important it is that we get electronic end-of-life records right. To do that we need to make changes both to digital systems and to practice so that people’s right to make decisions about their care is embraced and encouraged. The existence of the Palliative and End of Life Care Information Standard is an important step forward but its implementation will be critical to achieving real change for people approaching the end of life and for those close to them.
Dame Barbara Monroe
Summary
The impact on people and their care
In February 2021, Compassion in Dying and the Professional Record Standards Body (PRSB) carried out a national survey asking people to share their experiences of, priorities for and concerns about electronic end-of-life records. This report is based on an analysis of over 1,700 responses to the survey.
30% of people said they did not feel ‘at all confident’ that the healthcare team supporting or treating them would have access to their end-of-life wishes and preferences. Only 15% of people were ‘very confident’ that the healthcare team would have access to the information about their health that was needed when being cared for at the end of life.
The experiences people shared demonstrated five clear themes:
People experienced considerable anxiety about their wishes and health information not being known or acted upon when it mattered. People’s worries were based on:
previous bad experiences
a general lack of trust in NHS IT systems
concerns about their information not travelling between care settings or across geographical boundaries
People wanted to be more involved in viewing and editing their end-of-life records
People had bad experiences of end-of-life care when their wishes and health information were not known or acted upon by healthcare professionals
People had good experiences of end-of-life care when their wishes and health information were known about and respected
Recording their wishes was not always enough – many people needed ‘advocates’ to ensure their health information was known about and their wishes acted upon
A large majority of people either had concerns that end-of-life records would not work in the way they needed them to, or had an experience which showed that electronic end-of-life records did not enable key information to be known and shared when someone close to them was dying.
What people need from their electronic end-of-life record
People had strong feelings about what they wanted from their electronic end-of-life record:
88% of people said it would give them more confidence in their end-of-life care if the healthcare team supporting them could see what treatments they did and did not want
61% of people said viewing their end-of-life record on a website or app would make them feel more confident and 63% said they’d like to be able to make changes to their preferences via a website or app
69% of people said information about their health should be available to any healthcare professional supporting them whenever they need it, without having to give permission for the information to be shared, and 73% said the same for information about their wishes and preferences
For some, their wishes and health information being known was important because they had strong personal views about death and dying. Some wanted the comfort of knowing that what mattered to them would be understood by everyone. Others stressed the importance of it because previous experiences of illness or caring for a loved one had made them realise the impact that not knowing important information would have on their care.
People expressed very clearly what they needed an electronic end-of-life record to do in order for them to have peace of mind in the present and have what they considered to be a ‘good’ experience when receiving care and treatment in the last years, months or weeks of life:
Electronic records need to communicate people’s health information and end-of-life wishes seamlessly across care settings. People used the word ‘seamless’ frequently, and specifically mentioned sharing information between GP surgeries, paramedics, hospitals and care homes.
Electronic records need to travel between geographical boundaries. People cited experiences of receiving care and treatment at more than one hospital in different Clinical Commissioning Groups, or moving house or visiting family and needing to know that their health information and wishes would be instantly available in this new area.
At a minimum, people want to be able to view their end-of-life record to see what information is available to healthcare professionals. Some also want to be able to edit and update the information either themselves or alongside a healthcare professional. People expressed that being able to do one or both of these things would give them peace of mind, alleviate anxiety and enable them to live well with their condition.
Paper documents such as Advance Decisions or Do Not Attempt Cardio Pulmonary Resuscitation (DNACPR) forms must be easily visible in someone’s electronic end-of-life record to all healthcare staff. Furthermore, when people complete documents such as Advance Decisions to Refuse Treatment and share them with their GP, they want their GP to ensure that these documents are uploaded to their end-of-life record.
People want to feel reassured that a healthcare professional will have the time to look at their electronic record and that doing so is a routine part of their practice.
Moving forward
Simply having conversations is not enough to ensure that people’s wishes are known about and respected when it matters. It is equally important that those wishes are recorded in a way that can be shared and accessed by health and care professionals. Electronic end-of-life records are a valuable tool in bridging this gap, however as it stands people have little confidence in their records being shared appropriately.
The insights gained from this research should be vital in improving electronic end-of-life records. Keeping in mind why getting it right is so important to people and what difference this will make to their experience at the end of life has been central to the development of the new standard. We share these experiences to support healthcare leaders, trainers and commissioners to embed the new Palliative and End of Life Care Information Standard in a meaningful way into clinical practice. We hope these tangible examples will contribute to a culture where people are at the centre of decisions about their care.
Some definitions
Advance care planning gives people the chance to discuss, consider, plan and share their preferences for any future care while they still have the capacity to do so. This includes what medical treatments they might or might not want, their goals, values and what matters most to them. Ensuring that advance care plans are shared and accessible when they are needed is essential for palliative and end-of-life care to be delivered in a personalised way.
An electronic end-of-life record, previously called Palliative Care Coordination Systems (EPaCCS), is a digital record of key information relating to someone’s palliative and end-of-life care including advance care plans, CPR decisions, diagnosis, medications and other information that could be needed in an emergency. These electronic records enable the sharing of information between the healthcare professionals involved in someone’s care, often between multiple clinical settings.
A note on terminology: Throughout this document quotes have deliberately been kept in people’s own words, to reflect the language they use. Therefore different terms are used to mean the same thing, for example DNACPR (Do Not Attempt Cardio Pulmonary Resuscitation), DNR (Do Not Resuscitate) and DNAR (Do Not Attempt Resuscitation).
The research
In February 2021, Compassion in Dying and the PRSB carried out a national survey asking people to share their experiences of, priorities for and concerns about electronic end-of-life records. It also asked people what would make them feel more confident about their palliative and end-of-life care. Compassion in Dying shared the survey with the people they support and through Twitter. The PRSB circulated it to their wider health and care professional and patient stakeholder communities.
The survey was undertaken to inform the development of a revised Palliative and End of Life Care Information Standard1 setting out the content to be held in an electronic end-of-life record, which was published in June 2022. This Palliative and End-of-Life Care Information Standard has been developed as part of a wider programme of work by NHS England on digital palliative and end-of-life care, and the standard supports the newly published Universal Principles for Advance Care Planning.
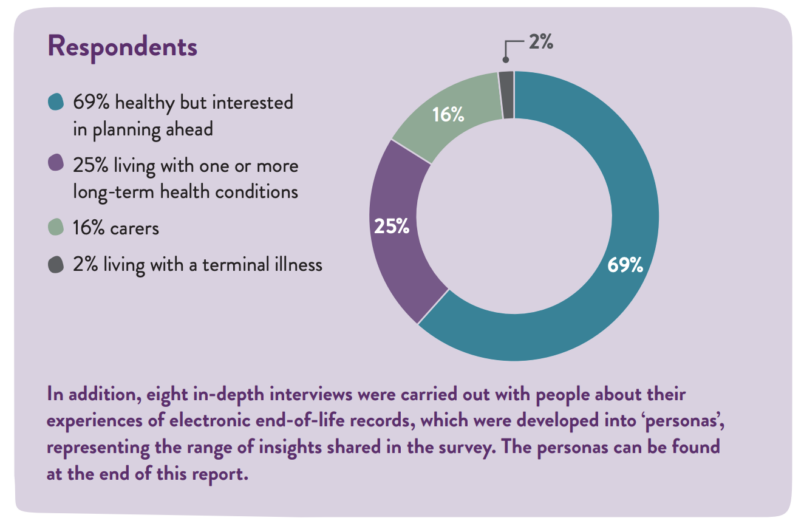
This report is based on an analysis of over 1,700 responses to the survey. People from 105 districts and counties across the UK responded to the survey. Of the 1,700 people who responded to the survey, 69% identified themselves as healthy but interested in planning ahead, 25% had one or more long-term health conditions, 16% were carers and 2% had been diagnosed with a terminal illness.
All quotes used are taken directly from the experiences people shared.
Findings
People experienced considerable anxiety about their wishes and health information not being known or acted upon when it mattered
This was the most common theme to emerge. People voiced serious concerns about their end-of-life wishes and health information not being known about when it mattered. This left people with anxiety about what treatment and care they would receive in emergency situations, for example, if paramedics were called to an accident. People were also concerned about what treatment and care they might receive if they lost capacity at the end of life, or were unable to speak for themselves. These concerns were present in people with existing conditions as well as people who identified as currently healthy.
For some people, anxiety about their wishes not being known came from having a bad experience in the past of their own or a loved one’s wishes and/or health information not being known or followed. For other people, anxiety about their wishes not being known came from a general lack of trust in the record-sharing systems currently in place.
People specifically worried about whether their health and care records would ‘travel’ with them between care settings e.g. between a GP surgery and a hospital, and between different areas in the UK. Again, some voiced this concern based on a previous bad experience of healthcare information not being available in different care settings, and others just had a general lack of trust in IT systems.
Numerous people also reported that they had no idea what happened to documents that they had completed which detailed their wishes for end-of-life care, once they had given those documents to a healthcare professional. This in turn caused anxiety. Several people reported experiences where they had given documents to their healthcare professional, but they were then lost, forgotten about or not uploaded properly onto their electronic end-of-life record. A lot of the worry expressed came from not being able to ‘see’ their medical notes or electronic end-of-life record, and people reported that if they could access the information in their record more easily it would give them peace of mind, which in turn would help them to live well now.
“I cared for my terminally ill husband until his death. I often felt there was a gap as to the information available to GP, palliative care and other healthcare professionals especially when out of hours care was needed. It was distressing to have to constantly be checking and checking again that the information was correct. It has not given me much confidence for my own end-of-life care. I’m a Stage IV cancer patient and this is a constant worry.”
People wanted to be more involved in viewing and editing their end-of-life records
Not being able to ‘see’ information on their electronic end-of life record resulted in anxiety and people wanted to be more involved in this. People specifically said that having access of some description to their end-of-life record would make them feel more in control and reduce anxiety. Some raised the idea of having an online tool or app where they could check details of their end-of-life wishes and health information and potentially edit them as they grew older, or as their health condition changed.
“As much as I’ve tried to make my wishes clear, I worry that this information won’t be seamlessly available. There seem to be a lot of shortcomings in the NHS regarding IT and the ability to share information between entities. Also, as a person with complex health and personal needs, that some important aspect won’t be passed on is a worry. I’d like to have the information in one place that I can see and amend if necessary and be confident that everyone is on the same page.”
“I could carry a note saying that this information is available from my GP, but it might be better if there was a standard card or notification that would be recognised by any healthcare professional. Ideally it should be available online so that they can access it at any time. I don’t know how much of my medical record and wishes are currently available in this way – I should like to know, and to be able to see it myself.”
People had bad experiences of end-of-life care when their wishes and health information were not known or acted upon by healthcare professionals
Large numbers of people told us about a bad experience of a loved one’s previously expressed wishes and health information not being known about or respected at the end of life. This often resulted in traumatic experiences for both the dying person and their loved ones.
Sometimes this was due to problems with paper forms detailing people’s wishes or health information being lost, or not being uploaded to an accessible electronic record which was transferable between care settings.
For others, even if their detailed plans were known about, it did not guarantee them getting the care that was right for them. Sadly, recorded wishes were sometimes not acted upon by healthcare professionals. This caused distress particularly to family and friends witnessing their loved one’s wishes being overlooked and subsequently receiving treatment they would not have wanted. This is significant because it shows that getting electronic end-of-life records right is not necessarily enough to ensure that the information in such a record is acknowledged and used.
“The paramedics repeatedly resuscitated my mother after a stroke despite her clear wishes and a DNR – I was present (and I have Power of Attorney). Because neither of us had paper copies of these documents with us, they and the hospital kept treating her invasively. She had signed the DNR at the same hospital before surgery a year before but it wasn’t on record. This was 2 years ago. She has been in a nursing home ever since and regrets daily, how, in her view, I failed her.”
“I was responsible for the care of my mother and aunt prior to their deaths 5 and 3 years ago. They were cared for in good-quality sheltered housing and nursing homes. Both had Advance Decisions and Advance Statements. They both had multiple admissions to hospital in their final few years. Their Advance Decisions NEVER got effectively communicated to hospital staff except when I physically gave a copy to them. In one case this resulted in treatment being given which should have been refused. I repeatedly tried to get the care home to instigate a better system.”
People had good experiences of end-of-life care when their wishes and health information were known about and respected
There were also a significant number of responses detailing good experiences of record sharing. When wishes were recorded and respected, people were able to have what they would describe as good deaths. For example, some people explained how having records shared meant not having to repeatedly talk to healthcare professionals across different settings about their loved one’s wishes at a time that is already stressful and upsetting. Others spoke about how having their own wishes shared effectively (e.g. when having an operation) has meant they trust that their wishes would be known about and respected in the future.
This demonstrates the importance of getting electronic end of-life records ‘right’. The impact on someone witnessing the death of a loved one whose wishes were known about and followed were in stark contrast to the experiences of those outlined in the ‘bad experiences’ section, and resulted in peace of mind for dying people and a more positive bereavement process for their loved ones.
“My late wife and I were very pleased and relieved that her clinical details and personal preferences could be recorded and shared across the organisations that might be involved in her end-of-life care. There was peace of mind that, if things happened at speed in an emergency, the records would be there for the professionals to access and understand without either of us having to give repeated instructions and so also alleviating the fear that personal preferences would not be implemented in a situation where the focus was on urgent care and care for the rest of our family in emotional and upsetting times.”
“As my wife’s life was coming to an end it was very comforting to know that the Marie Curie nurse attending was able to access all the information she required and see the DNR records.”
“My father was able to receive the end-of-life care he needed in the way he wanted without being transferred to hospital and without any of us having to worry that we didn’t know if this was his choice. We knew we were supporting the choices he made when he was able to make them and as a result we spent time with him rather than battling the healthcare system. Having his wishes pre-documented also ensured the staff were able to act confidently on his behalf too. Also none of us felt guilty or worried that we weren’t doing right for dad.”
Recording their wishes was not always enough – many people needed advocates to ensure their health information was known about and their wishes acted upon
Some people said that recording a person’s wishes for treatment and care was not always enough as they needed an informal advocate, like a family member or friend, to ensure their wishes were followed and key information known about. For example, many people detailed how they had to keep repeating what was in their loved one’s recorded care plan to healthcare professionals. For some, this was a difficult and stressful experience.
“My late husband had MND. The care he received in our local hospital was poor, nobody was prepared to look at his notes. I created and carried with me a folder with end-of-life stuff, DNR, Power of Attorney etc and made sure I watched as it was copied every time he was admitted then returned to me, to be sure it was all there and all in one place.”
“When I cared for dad, I had to rush after him to hospitals and clinics clutching the Advance Decision and Lasting Power of Attorney papers and making sure the carers passed them onto the hospital etc. It would have been so much easier if I could just have told them to check his records; the GP had them but they were rarely uploaded or updated. I’ve given my signed papers to the GP surgery but never heard if they have been uploaded to their system, I suspect not.”
“During the last year of his life, my father aged 88/89 had a couple of admissions to his local hospital A&E. I was amazed how they seemed to have no ready access to his medical records of any sort. Had I not been with him on each occasion, they would effectively have been dealing with a blank sheet of paper.”
Conclusion
Simply having conversations is not enough to ensure that people’s wishes are known about and respected when it matters. It is equally important that those wishes are recorded in a way that can be shared and accessed by healthcare professionals. Electronic end-of-life records are a valuable tool in bridging this gap, however as it stands people have little confidence in their records being shared appropriately. What is clear, is that when information is accessible to someone’s health and care team and known about when it matters, it has a hugely positive impact on that person’s end-of-life experience.
The insights in this report have been used by the PRSB and NHS England to inform the development of a new Palliative and End of Life Care Information Standard which sets out the content to be held in an electronic end-of-life record. The objective of the Standard is to ensure that clinicians have access to appropriate information to support decision-making for those with palliative care needs and those who are approaching the end of their life, through a personalised approach that aligns with what matters most to the person. The Standard supports the Universal Principles for Advance Care Planning2 which includes a principle on a person having shareable advance care plans, which record what matters to them, and their preferences and decisions about future care and treatment.
However, even the seamless sharing of electronic records will not be enough to ensure people’s wishes are always known about and respected. Having a perfect system for sharing end-of-life information relies also on healthcare professionals who are able to engage in advance care planning, know what to do when faced with someone’s electronic end-of-life record and respect the wishes contained in that record. The consequences of failing to do this are illustrated in some of the distressing experiences people shared in this report.
Alongside much needed changes to end-of-life records, there also needs to be increased focus on implementing recent policy which sets out so clearly how palliative and end-of-life care must be personalised and based on what matters to each individual. Healthcare professionals must be able to support people to consider and document their wishes and preferences, embrace people’s right to make decisions about their treatment and care, and be prepared to talk openly and honestly about death and dying. For healthcare professionals to do this they must be supported and trained properly to initiate conversations about planning ahead and recognise the cues from people that they might be open to talking about their wishes.3
It is also vital that people have access to honest information and are given the tools to ensure their wishes have been recorded properly. Compassion in Dying is supporting people to do this. Through our advocacy work we are enabling people and their loved ones to speak out when they feel their wishes are not being viewed as central in decision-making.
Getting electronic end-of-life records right is an important piece of the puzzle in ensuring people have the death that’s right for them.
The insights shared here lay bare why it’s so important – because getting it right makes people’s end of life experience better, and getting it wrong makes it much worse.
In the work that will follow the publication of the Palliative and End of Life Care Information Standard, it is vital that the views and experiences of patients and caregivers continue to be kept at the centre of everything. And we hope this report will enable decision-makers and front line staff to understand the varied needs of the people we all support.
Compassion in Dying is supporting this vital work by supporting people to:
consider what matters most to them
document their preferences in accordance with the Mental Capacity Act 2005
have the tools and confidence to advocate for themselves or their loved ones
and if necessary to challenge healthcare professionals if they feel that their or their loved ones’ wishes are being ignored at the end of life.
In 2019 we undertook research to see if GPs needed support with Advance Decisions, and developed new content specifically addressing their needs as a result. In 2020-21 we worked alongside the Care Quality Commission to enhance public understanding of DNACPR decisions and how they should be made. We continuously work with people in their communities to support them directly with advance care planning, and from 2020 we have been co-leads on a multi-partner advance care planning consortium in the London Borough of Lambeth working alongside diverse communities. We have also supported 71,000 people to make decisions about their treatment and plan their care through our nurse-led information line, our pioneering peer support service and our free online advance care planning service.
3 Compassion in Dying, Advance Decisions: Uncovering what GPs need, 2019
Personas
These personas are based on eight in-depth interviews with people on their experiences of Electronic Palliative Care Coordination Systems (EPaCCS).
My wife’s wishes and health information were known about when it mattered and this meant she had a good death
Ivan, 57, lives in London. His wife, Jude, died in 2018 when she was 48. They have three children. When Jude was being treated in hospital, with the support of her healthcare team she created a Coordinate My Care (CMC) Record and they also agreed on a DNACPR form. The plan was available to everyone treating her and gave Jude and her family peace of mind that her wishes and healthcare information were known about and would be respected. Ivan felt this contributed to Jude having a ‘good death’.
“My late wife, Jude, was diagnosed with a sarcoma in 2015 and had chemotherapy. When her diagnosis became terminal, Jude decided to refuse further treatment due to the potential side effects, and instead wanted to have the best quality of life possible in her remaining weeks.
Over the course of her illness, she was cared for at the Royal Marsden, where she then received palliative care. She was looked after very well, in a measured, respectful and loving way. While she was there we created a CMC record, and a DNACPR form.
Jude was thinking about being cared for at home, so the fact that paramedics and those caring for her in the community would have access to the CMC record and DNACPR form were really important to us. In the end, she found being at home too difficult, so went back to receiving palliative care in hospital.
Jude was happy to give consent to share her information once, while creating her CMC record, so that her clinical details and personal preferences could be seen by anyone that might be involved in her care, whether she was at home or in hospital. It was important that I didn’t have to be the person to relay that information as I was in the middle of my wife dying, while caring for our children. I had a lot to juggle and limited energy.
For us, it was important that it wasn’t just her clinical details that were shared, but also her other wishes. Particular details were important to us as practicing Catholics, for example, Jude wanted a priest to be present when she died.
Making a plan for what might happen right at the end gave her great comfort and knowing that everyone could see this information and would act on it was incredibly powerful. I think this helped Jude have a ‘good death’ because it gave her peace of mind that she’d made things easier for us, for me and the kids. Seeing Jude’s end-of-life care has shown me the importance of planning ahead and making my own wishes known. It has given me confidence that my own wishes would be known about by healthcare professionals if anything were to ever happen to me and I too take comfort in that.”
I have stage 4 cancer and I live alone so am really worried no one will know what matters to me
Faisal is 68 and lives in Wales. He was diagnosed with prostate cancer 4 years ago and is now under the care of a palliative care team. He also has a heart condition which he takes medication for. Faisal is particularly worried about whether healthcare professionals would be able to find out information about his healthcare and his wishes in an emergency because he lives alone and doesn’t have many close relationships.
“I have done an Advance Decision and a DNACPR form. Everyone has been given a copy of everything. But I haven’t seen proper proof that they are on my medical record. I worry that if I become incapacitated it would take anyone caring for me a long time to get information about me. They do have the information, but I’m worried about them finding it in a hurry or in an emergency.
If I had a stroke, which is likely, and couldn’t communicate, I’m not sure how long it would be before the hospital would see the right information. I’d like all those caring for me to have access to all information about my wishes and about my conditions.
I don’t have very long left and I know I’ll only need more care. I’m particularly worried about paramedics coming to my house. I’m worried that they would do something to keep me alive when it wasn’t appropriate because they can’t see what I want or don’t want. My daughter has a copy of everything but she lives in Cornwall so I couldn’t rely on her to get this information to those caring for me in an emergency.
I also live alone and don’t have many close relationships. There’s no one who really knows me well enough to fight my corner. Not even my GP could do this. It’s not like the old days when you’d have a GP who really knows you well. I don’t have anyone like that. At the moment, I feel really isolated because no one knows me intimately so my wishes probably wouldn’t be known about.
I have a history of depression too, which is on my medical records. It’s important to me that information about my mental health is on my medical record but sometimes I worry that healthcare professionals might make assumptions about me when they see information about my mental health so it’s important that healthcare professionals also see information about my wishes, and who I am as a person, to give them a more complete picture about who I am and why I don’t want treatment for cancer. Quality of life is the only thing I’m interested in, and I want those caring for me to know that but to also understand the reasons why this is important to me.”
My mum had dementia and received cancer treatment in different parts of the country but the right information was not available when it was needed at the end of her life
Ada is in her 50’s and lives in Lincolnshire. Ada brought her mum, who lived in Yorkshire, back to live with her so she could care for her at the end of her life. The different teams looking after her mum were across CCG boundaries, and did not share health records with each other. The lack of shared information had a big impact on her mum’s end-of-life experience.
“My mum lived with me during her end of life period. She had early dementia, went into hospital with a suspected stroke and when she was discharged she came to live with me. She’d had cancer in the past and so was referred to a cancer team in Hull. Different things were being followed up by different teams in different hospitals in different counties, which was confusing. There was no communication or record sharing between the hospitals – the different teams didn’t know which test had been done or what her diagnosis was.
We found out that she had terminal cancer in her brain. The end-of-life team where I live were brilliant because they had a shared electronic record so everyone that attended was well informed about the local care she was getting. This included her end-of-life wishes and healthcare information like her diagnosis and treatments.
The biggest issue was that because her oncology care had been provided in a different CCG, none of those records were available to anyone here. Nor were the hospital records. The end-of-life team had connections with the cancer team in Hull but they didn’t share electronic information. She was on a really rare medication, and she had a rare cancer, so every time healthcare professionals came to the house they were confused about the medication because they didn’t have access to information about her. Her dementia meant she couldn’t tell them the information they needed to know herself.
This caused a lot of additional work for me, as the various teams relied on me to provide answers and information. It was very stressful that I had to relay all the information. I was spending hours on the phone talking to them about medications and treatments. This is all while I was having to look after my mum at the same time. I feel this did compromise her care significantly, as mum experienced complex and apparently rare symptoms during the end of her life that were never really managed adequately.
If a single end-of-life record had been available, I think at the very least this would have improved communication between the different teams and would have improved the management of the difficult symptoms, making her end of life much less distressing and more peaceful than it was. It also would have been better for me – I wouldn’t have had to keep repeating things. They didn’t necessarily trust me because they needed to verify the information I was telling them. If there had been a single record, they wouldn’t have had to rely on me. Everyone would’ve had the right information at the right time.”
My husband had MND and no one at the hospital knew the right information when he was dying unless I told them myself
Sami is in her early 60’s and lives in Hertfordshire. Her husband died of MND 6 years ago. Towards the end of his illness he was unable to talk and couldn’t communicate his needs. Sami felt she had to be physically present at all times to advocate for him as she didn’t trust that key information would be known about. This felt like a big responsibility.
“My husband had MND. When he fell and was admitted to hospital, no one knew medical information about him. For example, they would leave a drink on the side and he wouldn’t be able to reach it because of his MND. I kept having to explain what he needed.
Also, the only way the hospital A&E knew his wishes was because I was there. Essentially, he just appeared at hospital and no one knew anything about him. They kept asking me whether I knew what his wishes were and I had to relay that information again and again. Luckily, we as a family had talked about it. We had a shared understanding of what his wishes were.
I created and carried with me a folder with paper copies of his end of life stuff, Advance Decision, DNACPR, LPA, because I didn’t trust that anybody had access to that information. I took it round with me any time he was admitted or moved. I would go to the desk and ask them to make copies and put them on his notes and flag them to all staff. I had to do this every time he was moved from department to department.
I did this because otherwise they wouldn’t know what he did and did not want. He was non-verbal. I could understand some of what he was saying because I knew him. If I wasn’t physically with him, none of his wishes were going to be known about. It gave me peace of mind to do this, because at least I knew that those caring for my husband would know about his condition and what that means for him. The MND clinic kept notes digitally. They were in a completely different league, I trusted them implicitly and I didn’t keep having to repeat information about his diagnosis and health needs like I did in the hospital.
I do think that carrying around his wishes and healthcare information made a positive difference to his death. This felt like a huge responsibility on my own even though my husband had shared his wishes with us in advance. It would have been much easier if the hospital had access to his wishes independently.
He said he didn’t want antibiotics, so in the end, nature took its course and I think he had a good death. But it felt awful having to say he shouldn’t have antibiotics when he had made those decisions himself already.
If that information could have been there, flagged electronically for everyone to see easily, and the people caring for him actually had the time to check and absorb it, it would have made the whole experience so much easier for me. I worry about what would have happened to him if he hadn’t had me there by his side all the time.”
I feel healthy but am getting older and worry my end-of-life record might have errors. If I could see it myself it would give me greater confidence as I get older
Ivy is 85 and lives in Bristol. She currently has no health conditions and feels healthy. She recently found out that there are errors and omissions on her medical records which has made her anxious that important healthcare information, and her wishes for end-of-life care won’t be known about when it matters.
“Last summer I went about making an Advance Decision. I spoke to my doctor about it and gave her a copy to put on my records. It’s important to me that it’s on my medical record because there’s no point in doing these things if it’s not going to end up being seen. Anyone who needs to see it should be able to have access to it to know what’s important to me.
I wish I was confident that the right people could see these wishes if I get ill or need treatment quickly. I have confidence that it’s somewhere in the system but I don’t have confidence that it will be shared without a phone call to the right person or even a letter being sent. The person who stands for me is my GP, so having her know my wishes makes me feel happier. I know I could talk to her about anything. But will a hospital or ambulance people know? I doubt it.
I’d like to be given a copy of the up-to-date information that is held on my end-of-life record. I know that there are errors and omissions on my health records during the time span August 2019 to April 2020, which I find disconcerting. I only saw it because it was part of GP referral documents needed for some medical insurance. I know what’s wrong with it, even though it was about a totally ordinary consultation about eye surgery. It makes me wonder what else is inaccurate on my health care records.
I truly wish my end-of-life record and the decisions and information it holds were routinely copied to me as the patient somehow. I want to see what’s there so I have a chance to correct it. I’d get a sense of freedom if I knew the right information was there, and that the right people could see it. There’s so much uncertainty as you get older and it would be lovely if this could be one of the things that I felt confident about. This would make me feel really supported and more in control of my health.”
I’m living with a long term condition and it’s important that information about my health and care wishes are available to all the different teams caring for me
Kay is 62 and lives in North Lincolnshire, where she moved a few years ago. She has endometrial cancer and a heart condition and is receiving chemotherapy and radiotherapy. She has an Advance Decision and a DNACPR form. Previously she has experienced mistakes on her medical record and a lack of information sharing between Trusts. This has made Kay worried about how her care will be coordinated in the future. She would feel more confident if health and care information was shared seamlessly between care settings, and if healthcare professionals proactively brought up and checked her healthcare information and wishes were correct and up-to-date.
“I had a hard time communicating with my late husband about what his wishes were, so I made sure my daughter wouldn’t have to guess what my wishes are. I’m very confident that my family are aware of my wishes.
It’s very important to me that my wishes are known about to the healthcare team caring for me because I’m at high risk of having a stroke and I really don’t want to be resuscitated.
On my medical records, it incorrectly states that I have angina – a mistake which was made 13 years ago. This came up recently when an anaesthetist was interviewing me before an emergency operation I was due to have. I have a paper copy of the report from my previous Trust which states that I don’t have angina but the anaesthetist wouldn’t accept a copy. It was really hard to get the two Trusts to talk to each other and they couldn’t see each other’s information.
I have various other conditions which didn’t come up in my pre-op interview, which makes me think my health information isn’t as complete as it should be. No one brought up my Advance Decision or DNACPR form before the operation either, which makes me think they couldn’t see either document. This information was all available to my GP but the hospital relied on me to tell them information. It made me really worried. I thought all my healthcare information and wishes for end-of-life care would be available to anyone caring for me. That’s what I want. If my heart had stopped during the operation, I’m sure they would have resuscitated me, even though I have a DNACPR form.
The mistake on my medical record delayed my operation. When you’re facing a diagnosis of any kind it’s so difficult. I was very frightened that I wouldn’t get the help I needed. While you wait, the cancer is progressing. It’s delaying treatment. I would have expected the hospitals and GP practice to talk to each other.
I would feel more confident if all healthcare professionals brought up my end-of-life wishes proactively. For example, my dentist asks me to initial her copy of my DNACPR form every 6 months. This makes me feel more confident that my wishes are known about and would be respected, and it gives me an opportunity to talk about my choices and wishes.”